Under the proposed rule, acute care hospitals that report quality data and are meaningful users of EHRs will see a net 2.8% increase in payments in FY 2024 (compared to 2023). However, disproportionate share hospitals could be facing a payment cut of $115 million.
While CMS says the 2.8% rise would increase hospital payments by $3.3 billion, the American Hospital Association (AHA) says it is not enough.
“The AHA is deeply concerned with CMS’ woefully inadequate proposed inpatient hospital payment update of 2.8% given the near decades-high inflation and increased costs for labor, equipment, drugs, and supplies. Moreover, long-term care hospitals would see a staggering negative 2.5% payment update under this proposal. These insufficient adjustments are simply unsustainable,” Ashley Thompson, AHA’s senior vice president for public policy analysis and development, said in a statement.
“2022 was the most financially challenging year for hospitals during the pandemic, with half of hospitals finishing the year with a negative operating margin. So far, this worrying trend has continued in 2023, most recently with reports of record high hospital defaults. The AHA has repeatedly requested that CMS and the Administration remedy shortcomings in its previous market basket forecasts for all hospitals, Thompson said.
For example, The AHA says CMS’ inpatient payment update was a full three percentage points less than what actual market basket inflation was in 2022 and the long-term care update was 2.9 percentage points less.
“Layering these inadequate inflationary adjustments on top of Medicare’s existing underpayments to hospitals does not reflect the reality of the world hospitals are providing care in. Without more substantial updates in the final rule, hospitals’ ability to continue caring for patients and providing essential services for their communities will be threatened.”
The Federation of American Hospitals piggy-backed on the AHA’s sentiment and called the update "disappointing."
“As the cost of groceries and gas continue to rise, so does the cost of caring for patients. Just as the ravages of record setting inflation are affecting every American family – community hospitals are being hit too. Hospitals aren’t immune to inflation. They are contending with rising labor costs combined with the growing challenges of a deepening caregiver shortage, drug price increases, and supply chain breakdowns, among other inflation challenges. All reasons why hospitals need more support from Medicare,” President Chip Kahn said in a statement.
“This IPPS proposed inflationary payment update is disappointing. It fails to recognize today’s headwinds that will strain the health safety net in 2024, which will further threaten patients’ access to care as hospitals are forced to reduce services or in some cases, especially rural areas, close completely.”
The IPPS proposed rule came at the same time that data from the AHA found that hospitals and health systems are dealing with an increase in financial pressures.
According to the AHA’s report, overall hospital expenses increased by 17.5% between 2019 and 2022, outpacing Medicare reimbursement, which only grew by 7.5% during the same period.
Labor costs, which typically account for half of a hospital’s budget, grew by 20.8% between 2019 and 2022. The growth in labor expenses was primarily the result of a rise in reliance on contract staffing. There has been a 258% increase in total contract labor expenses for hospitals in 2022 compared to 2019, according to AHA research.
Educating patients on how to navigate the billing process is essential in creating a positive patient financial experience.
April 23-29 is patient experience week, and HealthLeaders is helping to celebrate by spotlighting the hard work revenue cycle leaders put into creating a positive patient financial experience at their organizations.
During HealthLeaders’ Patient Financial Experience Summit last week, Mary Neal AVP of revenue cycle at Ochsner Health, and Savanah Arceneaux, director of pre-service and financial clearance at Ochsner Health, chatted with me during a summit session about how to create and streamline patient education resources in order to increase patient satisfaction among challenges such as the No Surprises Act.
Between complex billing statements and good faith estimates, revenue cycle staff have a lot on their plate when it comes to helping patients navigate these multifaceted and arduous statements. And at a time when a poor financial experience can negate a five-star clinical experience, revenue cycle leaders are under more pressure than ever to streamline processes for their patients.
So what are the keys to remedying this? Neal and Arceneaux say it ties back to patient education on all aspects of the revenue cycle, but payer and cost education can make the biggest difference.
“In recent years, payers began shifting more financial responsibility to the patients, and that's been a big challenge. This has really prompted us to look at our long-term strategic vision for how we can make this experience more consumer friendly by opening that digital front door and giving patients various options for them to gain resources and education on their plans,” Arceneaux said.
This has led Ochsner to embrace services and technology that get them closer to the patients and make that connection before they even come in for their visit.
“It can be challenging being a patient-centered organization while we are attempting to collect what is being owed to us, so we want to be able to do this while involving our patients at every step. We want them to be financially informed prior to their visits so that they are feeling satisfied when they come in,” Arceneaux said.
Another way of doing this is providing education around their good faith estimates as well.
“If you can get in touch with the patient two, three, or four weeks ahead of their service and provide them a proactive estimate of their service cost, that allows a lot of time for our staff to research questions, maintain a dialogue about pricing, and help the patients understand,” Neal said.
“It really helps to break things down for the patient prior to services rendered, so you can avoid the ‘here's your bill, this is what you're stuck with now.’ When that happens, there's a little bit less recourse and it can make the patients feel powerless since they've already had these services rendered,” Neal said.
Interested in improving the patient clinical experience too? Make sure to also check out the educational session, How to Improve HCAHPS Scores, which features Ghazala Sharieff, MD, MBA, corporate senior vice president of hospital operations and chief medical officer at Scripps Health as well as Brooke Horne, MPH, executive director of patient experience at Providence.
Sharieff and Horne discuss a range of issues related to improving HCAHPS scores. Two of the top topics are improving physician and nurse communication scores.
Revenue cycle leaders were asked to rank the most time-consuming tasks at their organization, and the results aren’t surprising.
556 chief financial officers and revenue cycle leaders at hospitals and health systems across the United States were asked to rank the most time-consuming revenue cycle tasks at their organizations in a new survey commissioned by AKASA.
Topping the list of the most time-consuming revenue cycle tasks were denials management and prior authorizations.
In the survey, respondents were able to select up to five out of a list of 15 different revenue cycle tasks. Of the tasks listed, the following five were selected the most by the leaders:
76%, denials management
60%, prior authorization
58.6%, insurance follow-up
26.6%, eligibility and medical necessity checks
26.4%, patient cost estimation and price transparency requirements
Seeing denials management at the top of the list is no surprise as HealthLeaders has dubbed 2023 as the year of reducing denials for revenue cycle. An abundance of recent studies have been pointing to the growing concern of denials for revenue cycle leaders as more pressure is put on these leaders to help increase their bottom lines.
As denial rates continue to increase, establishing a streamlined denials management strategy is key for healthcare organizations to reduce complexity and workload for staff and avoid reimbursement delays, AKASA noted.
“When thinking about the biggest bang for your buck as a revenue cycle leader, few things are as effective as focusing on denials management,” said Amy Raymond, VP of revenue cycle operations at AKASA, said in a statement shared with HealthLeaders.
“But it’s important to avoid the common mistake of only focusing on working denials, and instead address the root causes. Leveraging robust, AI-driven automation can help overcome shortcomings of a typical denial management strategy—improving processes holistically to reduce denials in the first place and better address them when they occur,” Raymond said.
Seeing prior authorizations at the top of the list is of no surprise either, especially since prior authorizations are having a large impact on denials. In fact, a separate study earlier this year highlighted the burden prior authorization denials have had in the revenue cycle in 2022.
According to that study, denials rose to 11% of all claims last year, up nearly 8% from 2021, and prior-authorization denials were at the heart of the cost increase. Prior authorization denials on inpatient accounts were a key driver behind the dollar value of denials increasing to 2.5% of gross revenue in August 2022 up from 1.5% of gross revenue in January 2021—an increase of 67%, according to the report.
Clinical validity denials occur when there is a lack of clinical evidence in the patient chart to support a billed diagnosis. Claims may be denied, for example, if they lack clinical criteria necessary to support a diagnosis, contain inconsistencies, or do not meet payer-specific diagnostic criteria.
A key defensive strategy for preventing these denials is provider education, Reck said. This can involve bringing data on the financial impact of documentation inconsistencies to providers and explaining how they can be prevented. Streamlining this process to avoid these clinical validation denials will help to lessen the burden of overall denials management.
The list ranks the top-performing hospitals across the U.S. by net patient revenue.
A report published earlier this year by Definitive Healthcare ranked the nation’s top-performing hospitals by net patient revenue. As revenue cycle leaders know, to thrive as an organization, a streamlined and optimized revenue cycle is a must. Every area from the front end to the back end need to be well aligned and working efficiently.
As a key indicator of a healthcare organization’s financial strength, many thought leaders believe increasing net patient revenue to be one of the most difficult challenges hospitals face nationwide, the report noted.
Fluctuating patient volumes, decreasing reimbursement rates, and constant pressure to keep up with changing regulations as the reasons why improving financial performance is such a struggle, it said.
Hospitals calculate net patient revenue by subtracting deductions such as charitable donations, bad debt, and contractual adjustments from the gross revenue received for all patient care performed, the report noted. According to the report, the following data is displayed and ranked according to the most recent 12-month interval tracked in its database.
Here are the top five hospitals on the list along with net patient revenue:
Tisch Hospital, $6,273,707,636
Cleveland Clinic Main Campus, $6,037,196,525
NewYork-Presbyterian Weill Cornell Medical Center, $5,734,047,089
AdventHealth Orlando, $5,004,081,001
Vanderbilt University Medical Center, $4,691,813,631
Many hospitals on the list are bringing in billions of dollars in net patient revenue with the top ten reporting over $3.9 billion, the report said. Combined, the top 50 hospitals earned more than $151 billion in net patient revenue, while the average hospital earned roughly $3.03 billion.
395 new diagnosis codes have been proposed by CMS for fiscal year 2024.
CMS recently released the fiscal year 2024 inpatient prospective payment system proposed rule, and with it came the annual proposed ICD-10-CM diagnosis code changes which include new codes to enhance the tracking and progression of Parkinson’s disease and more reimbursement for certain social determinates of health (SDOH).
The proposed rule includes 395 additions, 12 revisions, and 25 deletions to the ICD-10-CM diagnosis code set. If finalized, these changes will take effect October 1.
Of the 395 new ICD-10-CM codes, 123 of them are external cause codes to capture accidents and injuries. CMS also proposes 36 new codes for osteoporosis with current pathological pelvic fracture.
Other notable proposed code additions include:
Several new codes for sickle cell anemia
Five new codes for Parkinson’s disease with and without dyskinesia
Four new codes for migraine with aura
Three new codes for insulin resistance
When it comes to SDOH, the proposed changes would create two codes that indicate if a caregiver’s noncompliance is due to financial hardship or another reason. For example, the current code for “caregiver’s other noncompliance with patient's medication regimen” would become invalid and coders would use Z91.A41 (Caregiver's other noncompliance with patient’s medication regimen due to financial hardship) and Z91.A48 (Caregiver's other noncompliance with patient's medication regimen for other reason).
In the proposed rule, CMS also recognizes homelessness as an indicator of increased resource utilization. To compensate acute care hospitals for resources needed to care for patients experiencing homelessness, CMS proposes to increase the severity designation of three ICD-10-CM codes describing homelessness.
CMS invites the public to comment on all proposals. For more information on the rule, see the Federal Register. Comments are due to CMS no later than June 9.
Under the proposed rule, acute care hospitals that report quality data and are meaningful users of EHRs will see a net 2.8% increase in payments in FY 2024 (compared to 2023), an expected increase of $3.3 billion. However, disproportionate share hospitals could be facing a payment cut of $115 million.
Under this rule, hospitals may be subject to other payment adjustments under the IPPS, including:
Payment reductions for excess readmissions under the Hospital Readmissions Reduction Program
Payment reduction of 1% for the worst-performing quartile under the Hospital Acquired Condition Reduction Program
Upward and downward adjustments under the Hospital Value-Based Purchasing Program
CMS is also proposing health equity adjustments under the Hospital Value-Based Purchasing Program, which adjusts IPPS payments to acute care hospitals depending on their quality performance in the inpatient hospital setting. As part of its goal to measure policy impact more explicitly on health equity, CMS has proposed adding 15 new health equity hospital categorizations for payment impacts.
Hospitals may also see higher payments under a proposal to recognize homelessness as an indicator of increased resource utilization in the acute inpatient hospital setting. CMS proposed changing the severity designation of three ICD-10-CM diagnosis codes that describe homelessness from “non-complication or comorbidity” to “complication or comorbidity” to address the higher average resource costs of cases with these codes.
CMS has also proposed to allow rural emergency hospitals to be designated as graduate medical education training sites. This would enable more medical residents to train in rural settings amid worsening clinician shortages, especially in rural communities, CMS said.
Revenue cycle leaders should review the proposed rule and analyze the proposals’ potential impact on reimbursement and workflows. Changes could have a cross-functional impact, so it’s always important leaders ensure that all revenue cycle departments are aware of the proposed changes.
An enhanced EHR is key to a healthy revenue cycle, but one CMO says clinicians can't be left out of decision making and optimization.
HealthLeaderspreviously spoke with Michael Weiner, CMO of MSU Health Care, in East Lansing, Michigan, about a range of topics, including post COVID-19 clinical challenges and physician leadership, but there was one topic discussed that has been top of mind for revenue cycle leaders: optimizing the EHR.
HealthLeaders asked if there was anything specific that can be done to EHRs to make them more user friendly for clinicians, and according to Weiner, including clinicians in optimization and decision making is key.
“For example, when I see a patient, if I have to click 40 times to get from the beginning of the patient encounter to the end of the patient encounter, is there a more optimal way to do that? Is there a way to get through in 20 clicks? Is there a way for me to be able to dictate into the blocks I need to fill out to make it more efficient for me?” Weiner asked.
One solution Weiner said is offering advanced optimization training, which is having elbow-to-elbow experts working with the physicians as they see patients to improve their workflow within the EHR. Doing so will not only help the clinical team, but the patients too.
“There are also technologies that can make the experience better for clinicians and patients. We have adopted patient-supportive technology to make it easier to sign in, to make it easier to give medical history, and to avoid filling out pages of forms when you see a doctor. You can also bring in additional support such as scribes to help do the input work. We are looking at optimizing the electronic health record to improve retention and to make us a more attractive employer,” Weiner said.
When revenue cycle leaders look to update, implement, or optimize this software, the importance of including input from the clinical team was recently echoed by Liza Dzhezhora, healthcare IT analyst at Itransition.
“An EHR project’s success depends on more than just qualified developers; it also requires clinicians with industry-specific knowledge of hospital tasks, operations, and workflows. Hence, the EHR implementation project needs both technical and clinical perspectives,” Dzhezhora said.
According to Dzhezhora, revenue cycle leaders should select doctors with medium to high levels of computer competence (superusers), singling them out with the help of online tests. During the project, superusers should perform four essential tasks:
Workflow mapping. Superusers can map the selected workflows and regularly update them to make sure they fully reflect clinical processes.
Drafting the needed integrations. Through their awareness of existing digital solutions, superusers can map the necessary integrations and provide the information to the development team.
Usability testing. Superusers can identify issues that are potentially dangerous for patients, like wrong dosages or units of measurement.
Mentoring. Superusers can oversee beginners’ training, helping them master workflows and daily tasks.
“Doctors’ participation in the project can improve all clinicians’ understanding of the new EHR system and its place in their organization while making the implementation smoother,” Dzhezhora said.
The revenue cycle moves quickly, and so does its news.
Nearly 17% of in-network claims were denied by ACA marketplace plans in 2021.
Health insurers on the Affordable Care Act (ACA) marketplace denied an average of 16.6% of in-network claims in 2021, according to a brief by Kaiser Family Foundation.
Researchers analyzed data released by CMS on claims denials and appeals for qualified health plans (QHP) offered on HealthCare.gov for the 2021 plan year and found that denial rates ranged significantly from 2% to 49%. The dataset included 162 QHPs that reported receiving at least 1,000 in-network claims and showed data on claims received and denied.
Two out of three patients have never disputed a medical bill.
Patients don't usually contend medical bills, but when they do their chances of getting charges removed or reduced are high, according to a YouGov survey commissioned by revenue cycle firm AKASA.
Over 2,000 Americans were polled between March 9-14, 2022, including 179 adults with employer-sponsored high-deductible health plans, to gauge patient experience with disputed medical bills.
Nearly two-thirds of respondents (64%) reported having never challenged the validity or accuracy of a bill with their physician, hospital, or health insurance company. That figure shot up to 78% for uninsured individuals, while those with high-deductible health plans (45%) and Medicare Advantage (43%) were more likely to contend bills.
Healthcare execs eye workforce and back-office solutions in new AI study.
A new survey on the use of AI in healthcare finds that roughly half of the health systems surveyed are using the technology for back-office operations and workforce issues, and there's a lot of interest in conversational applications.
The survey of 40 leading healthcare executives, conducted by The Health Management Academy, sees growing support for AI "to fill gaps and improve productivity," according to a press release accompanying the report. And that growth is coming fast: Almost 85% of those now using AI for workforce issues expect a moderate to significant increase in one to three years.
Critical access hospitals, rural emergency hospitals, and other rural facilities should all take note of updated CMS guidelines.
As we know, it is essential for revenue cycle leaders to remain informed and compliant with the ever-changing CMS guidelines to ensure efficient reimbursement processes.
That being said, CMS recently released guidance on the proper billing practices, designations, and conversion processes for critical access hospitals (CAH) and rural emergency hospitals (REH). Remaining compliant with these designation and conversion processes will ensure your organization is getting the reimbursement it deserves.
Medicare-participating hospitals must meet several conditions to become and remain a CAH. CMS updated the location requirement for CAHs, specifying that they must be more than a 35-mile drive on primary roads from any other CAH or hospital.
A primary road is a numbered federal or state highway with two or more lanes each way, according to the guidance. CAHs in areas with only secondary roads available or mountainous terrain must be a 15-mile drive from other hospitals.
To establish a process for overseeing and resolving patient grievances, CAHs are now required to inform each patient of their rights before starting or ending care. In addition, CAHs must now have a unified and integrated quality assessment and performance improvement program if they are part of a multi-hospital health system.
The updated guidance also detailed the optional payment method for CAHs. “Under the optional payment method, the CAH bills facility and professional outpatient services only when physicians or practitioners have reassigned their billing rights to them,” said CMS. After physicians and practitioners reassign their billing rights to a CAH, they can’t bill for professional services.
CMS also included information on its newest provider type, REH. “REHs allow for emergency services, observation care, and additional medical and health outpatient services (if the REH elects to provide them) that don’t exceed an annual per-patient average of 24 hours,” said CMS.
REHs generally convert from a CAH or rural hospital with no more than 50 beds and don’t provide acute inpatient services, according to CMS.
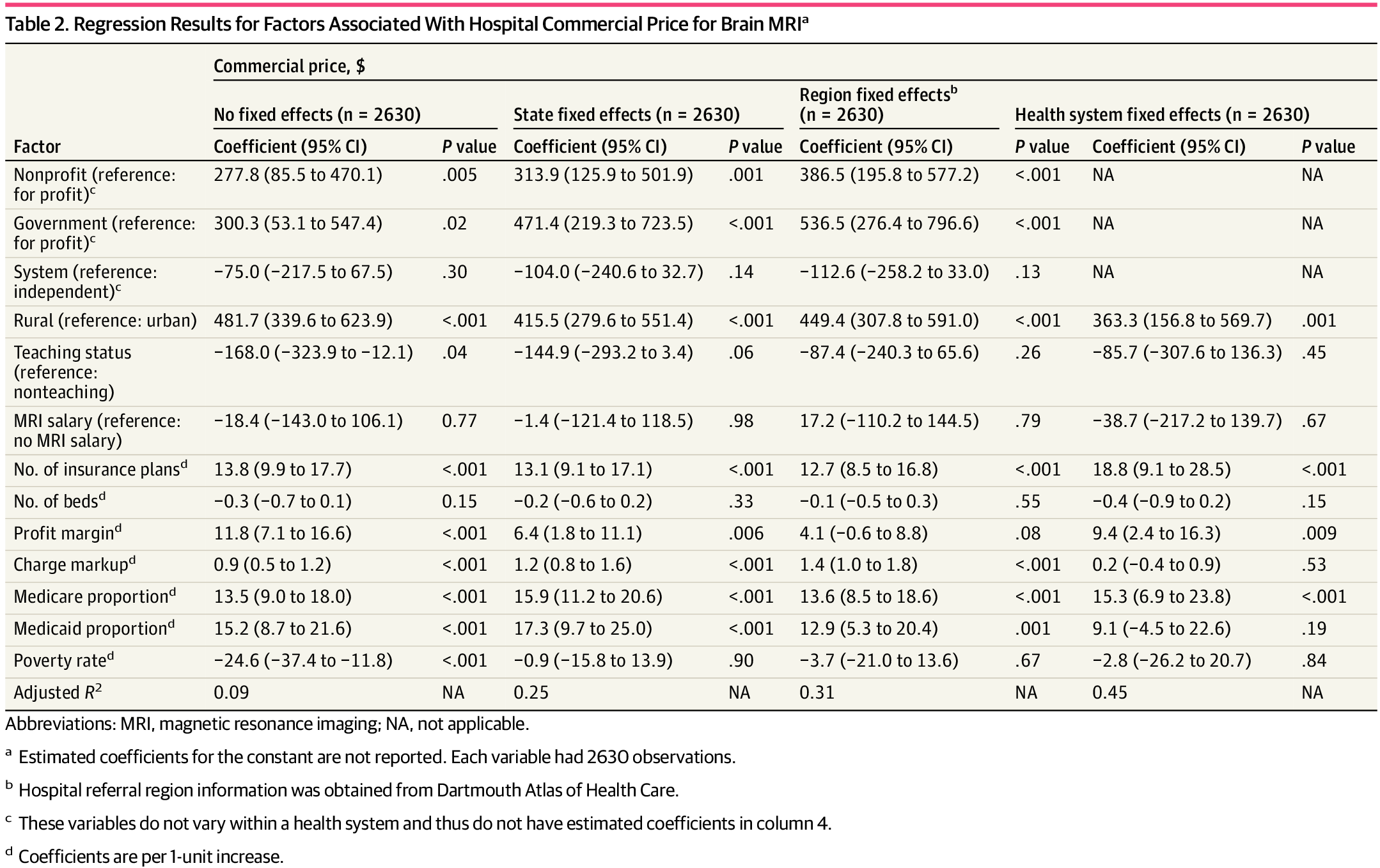
A new study shows nonprofit and government hospitals have higher commercially negotiated prices for MRIs than for-profit hospitals.
A study published in JAMA Open Network examined negotiated rates under the price transparency rule and has identified the most expensive type of hospital to receive a brain MRI among those that complied with the rule as of June 13, 2022.
The study leveraged new data associated with commercially negotiated prices nationwide to compare commercial rates for MRIs of the brain before and after contrast reported with CPT® code 70553. According to the study, nonprofit and government hospitals had higher commercially negotiated prices for brain MRIs than for-profit hospitals.
“Across the nation and within the same state, referral region, or health system, hospitals located in rural areas, contracting with more health plans, or treating more Medicare patients had higher prices, potentially reflecting these hospitals’ stronger bargaining power compared with insurers in their local markets,” the study said.
The sample contained 2,630 hospitals and found the following:
The median commercial price was $1,900 for nonprofit, system-affiliated hospitals in urban areas
Prices at nonprofit and government hospitals were $387 and $537 higher than the prices at for-profit hospitals
Photo courtesy of JAMA study ‘Factors Associated With Hospital Commercial Negotiated Price for Magnetic Resonance Imaging of Brain’
Since the hospital price transparency regulation went into effect on January 1, 2021, hospitals are required to make public their standard charges for items and services through a consumer-friendly display showing at least 300 shoppable services, as well in a machine-readable file.
Hospitals were slow to adapt out of the gates. In an assessment of 235 randomly sampled hospitals conducted by CMS between January and February 2021, 66% met consumer-friendly display criteria, 30% posted a machine-readable file, and 27% did both.
Those figures improved significantly in CMS' second assessment, this time of 600 randomly sampled hospitals between September and November 2022. The analysis found 493 hospitals (82%) posted a consumer-friendly display, 490 (82%) posted a machine-readable file, and 421 (70%) did both.






ae17.jpg)